Health Management
Solutions
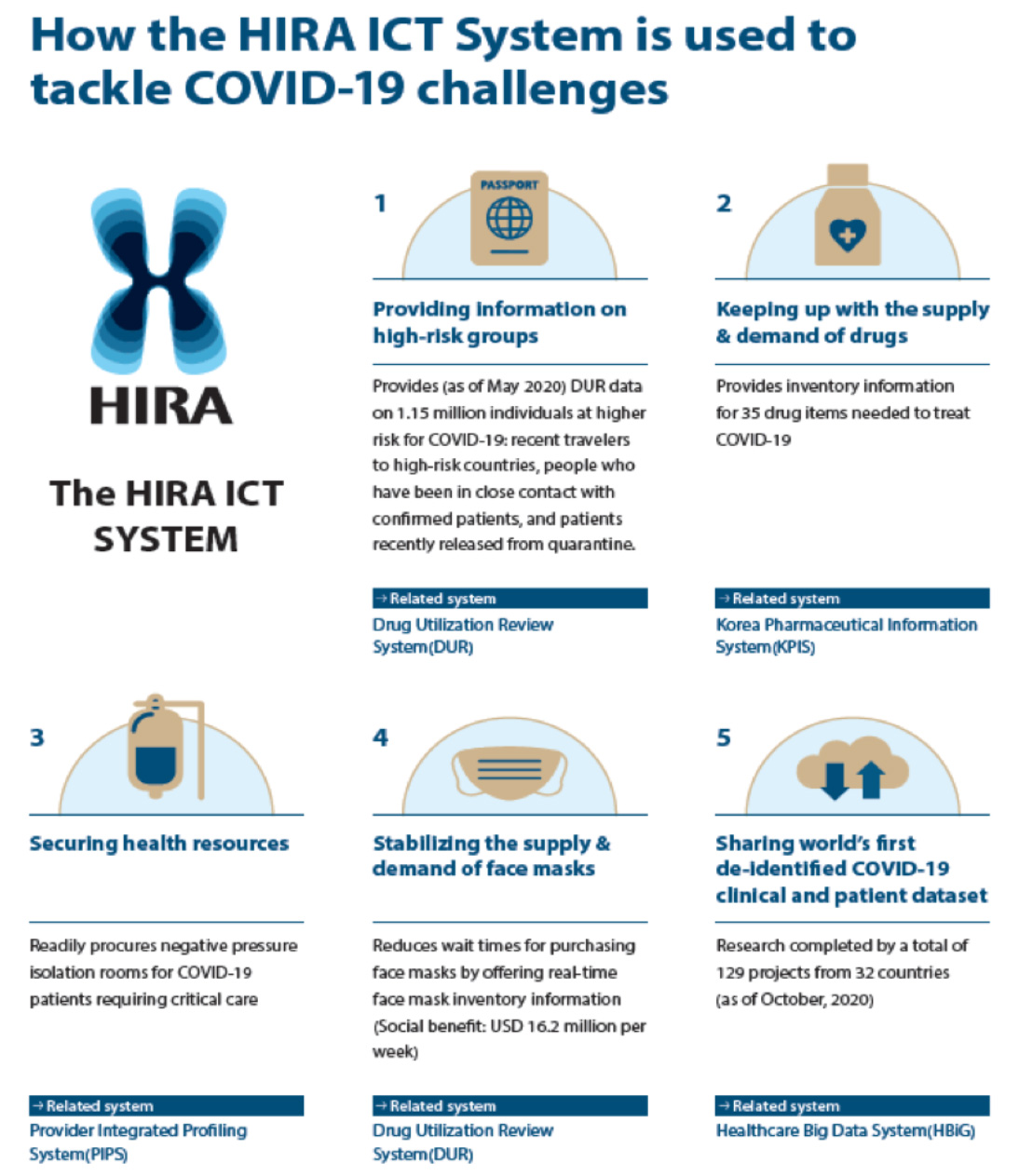
The use of ICT technologies, such as the Self-check Mobile App and Self-Quarantine Safety Protection App reduced administrative burden and allowed the Koreans to follow the national response measures more easily. During the MERS outbreak in 2015, the Drug Utilization Review (DUR) system was served to provide real-time information about those who entered Korea related to infectious disease. In 2018, the upgraded International Traveler Information System (ITS) was installed in the DUR system to establish a systematic platform for medical institutions. This system was enabled identifying their patient’s travel history from the stage of reception into institution (MOFA, 2020).
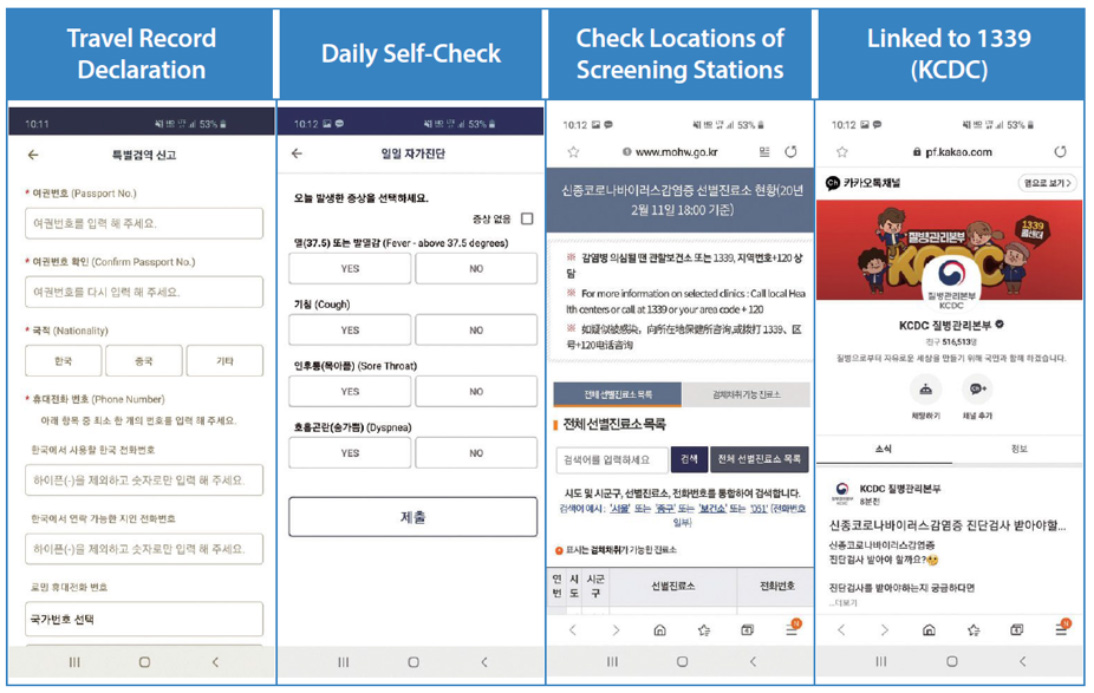
① a screen where the user under the Special Entry Procedure is requested to enter information (such as passport information, nationality, contact information)
② a screen where the user conducts self-check of symptoms such as fever, cough, or sore throat and submits the results once a day (for up to 14 days after entering the country)
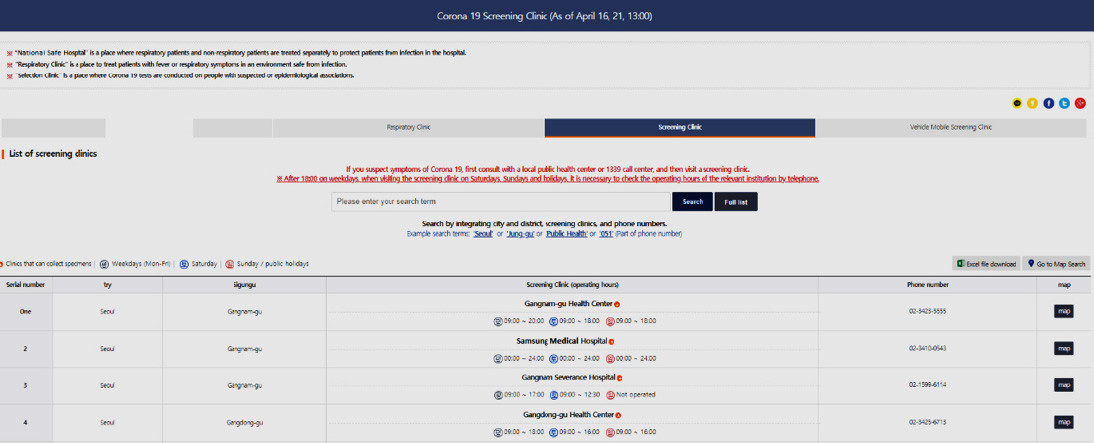
③ a screen directing the user to the KCDC 1339 Call Center/social media counseling channel and offering information on nearby screening
stations.
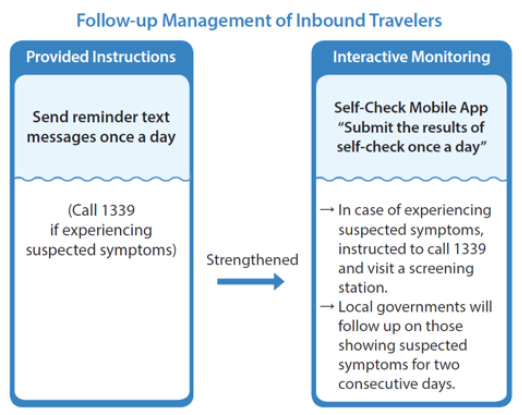
All inbound travelers are to install the App, check their condition for possible symptoms, and submit their self-check once a day for 14 days, starting from the date of entry. In addition, the list of all inbound travelers is provided to each local government, enabling the local authorities to strengthen the monitoring system.
* Self-check conducted for the following symptoms: fever (over 37.5℃), cough, sore throat/throat pain, difficulty breathing/shortness of breath
The Korean government advised inbound travelers to call the KCDC 1339 Call Center if they experienced suspected symptoms during their stay in Korea, using the contact information of the Call Center shown on the traveler’s Special Health Declaration.
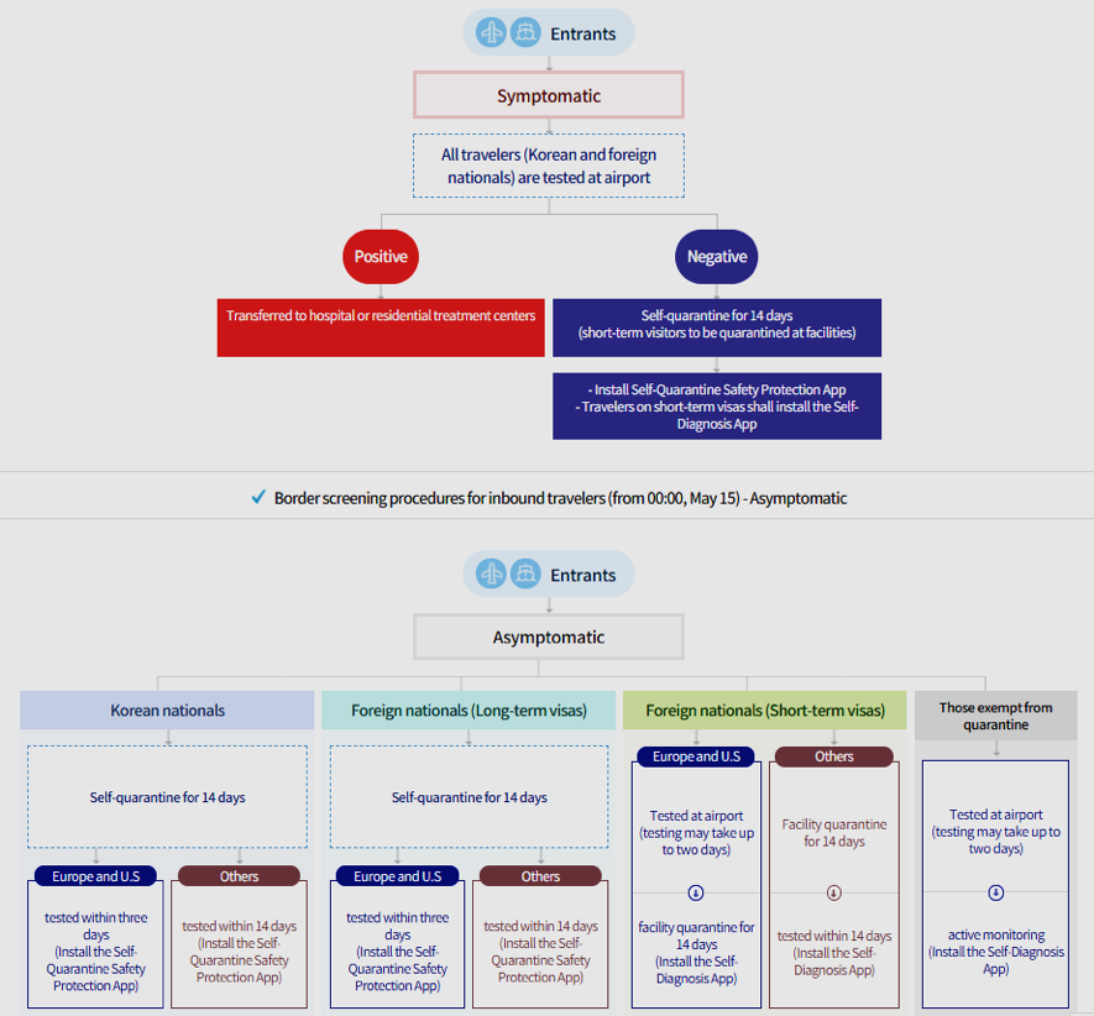
“all inbound travelers (Korean and foreign nationals) receive temperature screening and fill out the Health Questionnaire and Special Quarantine Declaration in accordance with the Special Entry Procedure. All travelers subject to the special procedure are allowed to enter the nation after their contact information and address of residence in Korea is verified. They are also required to install either the “Self-Quarantine Safety Protection App” or “Self-Diagnosis App” on their phones to monitor if they show symptoms that indicate infection of COVID-19 such as fever during their stay in Korea. All inbound travelers must install either of the two applications, to check their health status and record if they develop any symptom on a daily basis for 15 days beginning from the day of arrival. In addition, the list of incoming travelers is provided to each local government (city or province) in an effort to strengthen the monitoring system.”

- The doctor sends the details of prescription to HIRA DUR service before issuing the prescription to the patient. HIRA sends a warning message in a pop-up window on the doctor’s computer screen within 0.5 seconds, in case there is a risk factor in the prescription when compared to the patient’s medication history, suspended drug list, and DUR standards. The doctor could choose to change the prescription or to proceed with the original prescription with a memo, explaining why the drug should be used exceptionally. The final prescription information is sent to and stored in the DUR system of HIRA
- Pharmacists undergo the same process at the pharmacy when dispensing. For a warning message, the pharmacist could choose to change, or go ahead with the original prescription after checking with the doctor. The final dispensing detail information is sent to and stored in the DUR system of HIRA


“Application programming interfaces enable information systems to communicate and transfer data among each other. Depending how it is configured, an API can enable a system to send or retrieve data that can update an individual’s record or provide collective data that can be used to create reports. An API also can send information from one system to another. A healthcare provider organization, for example, can input a patient’s information into a system that works with insurance companies and nearly automatically determine the patient’s coverage for a specific procedure or medication.” (Healthcare IT News, 2019).